Meta-analyses of the efficacy of asenapine versus placebo in bipolar i disorder as monotherapy and adjunct therapy compared with other atypical antipsychotics
СтатьиHein Fennema,1 Bernhard Slaap,1 Armin Szegedi2
Introduction
Antipsychotics have demonstrated efficacy as both monotherapy1 and adjunct therapy2 for acute bipolar mania.
Asenapine is an antipsychotic with a unique pharmacological profile approved in the united states for treatment of schizophrenia, and for acute treatment as monotherapy or adjunctive therapy to lithium or valproate, of manic or mixed episodes of bipolar l disorder in adults.3 In the European union, asenapine is approved for the treatment of moderate to severe manic episodes associated with bipolar l disorder in adults.4
Flexible-dose asenapine (5 or 10 mg twice daily [BID]) has demonstrated efficacy for acute bipolar mania as monotherapy in 2 placebo- and olanzapine-controlled monotherapy trials (A7501004 [NCT00159744] and A750100[NCT00159796])5,6 and as adjunctive therapy in a placebo-controlled trial in patients with incomplete response to lithium or valproate (A7501008 [NCT00145470]).7
We report the results of meta-analyses of the relative efficacy of asenapine versus other antipsychotics in the treatment of acute mania as monotherapy or adjunctive therapy to lithium or valproate using all available randomized, short-term, placebo-controlled clinical trials.
Objective
To further assess the relative efficacy of asenapine as monotherapy and adjunctive therapy to lithium or valproate compared with other antipsychotics based on placebo-controlled trials using meta-analyses.
Methods
Search Strategy and Study Inclusion
All available randomized, short-term (3 or 12 wk), placebo-controlled data from the asenapine bipolar I disorder program were included in the analyses; 2 of these trials included olanzapine data.5,6
We identified randomized, short-term (3-6 wk), placebo-controlled clinical trials of other antipsychotics as monotherapy or adjunctive therapy to mood stabilizers in adults with bipolar mania published from 1999-2009 (a range deemed to be appropriate for clinical trial publications of antipsychotics for bipolar I disorder) based on the methods of Perlis and colleagues.8
PubMed and MEDLINE searches were conducted using the search terms "mania" and "placebo" combined with aripiprazole, olanzapine, quetiapine, risperidone, or ziprasidone; relevant meeting abstracts were also included.
The primary endpoint across trials was generally change from baseline at week 3 on Young Mania Rating Scale (YMRS) total score versus placebo; all ziprasidone trials (n=4) used the Mania Rating Scale and 2 olanzapine studies used 4 or 6 week endpoints (see † and ‡ in the Summary of Studies Table).
Data Analysis
Data from asenapine clinical trials at the effective dosages of 5 or 10 mg bid were assessed using the prespecified primary analyses,5-7 with treatment differences estimated using analysis of covariance adjusted for baseline YMRS value and (pooled) investigative site; last observation carried forward was used to impute missing data.
Meta-analyses were performed on change from baseline ymrs total score at endpoint versus placebo; each active agent was compared with placebo from the same study.
Meta-analyses used the random-effects model described by DerSimonian and Laird9 to determine average treatment effects and associated 95% Cls.
Testing for an equal effect of compounds in monotherapy studies was done using a 2-stage meta-analysis."
In the first stage, the Dersimonian and Laird9 method was used to estimate the variance across studies within compounds. In the second stage, all individual studies were included nested within compound, using the variability estimates of the first step for each study. This regression model provides an overall test of equal treatment effect of compounds.
The Cochran Q statistic was used to assess homogeneity across studies.
Data from 19 monotherapy and 9 adjunctive therapy trials were included in the analyses.
| Monotherapy Trials | |
| Asenapine | McIntyre RS, et al. Bipolar Disord. 2009;11(8):815-826; Mcintyre RS. et al .J Affect Disord. 2010;122(1-2):27-38 |
| Aripiprazole | McQuade RD, et al. Aripiprazole vs placebo in acute mania: safety and tolerability pooled analysis [poster), Presented at 5th International Conference on Bipolar Disorder; June 12-14, 2003; Pittsburgh, PA*; Keck PE, Jr., et al. Am J Psychiatry. 2003;160(9):1651-1658; Sachs G, et al. J Psychopharmacoi. 2006;20(4):536-546; Keck PE, et al. J Affect Disord. 2009;112(1-3):36-49;Young AH, et al. Br J Psychiatry. 2009;194(1):40-48 |
| Olanzapine | Tohen M, et al. Am J Psychiatry. 1999;156(5):702-709; ‡Tohen M, et al. Arch Gen Psychiatry. 2000;57(9):841-849; Tohen m, et al Clin Psychiatry. 2008;69(11):1776-1789 |
| Quetiapine | McIntyre RS, et al. Bur Neuropsychopharmacol. 2005; 15(5):573-585; Vieta E, et al. Curr Med Res Opin. 2005;21(6):923-934; Bowden CL, et al. J Clin Psychiatry. 2005;66(1):111-121 |
| Risperidone | Hirschfeld RM, et al. Am J Psychiatry. 2004;161(6):1057-1065; Smutevich ab, et al. Eur Neuropsychopharmacol. 2005;15(1):75-84; Khanna S, et al. Br J Psychiatry. 2005;187:229-234 |
| Ziprasidone† | Keck PE Jr, et al. Am J Psychiatry. 2003;160(4):741-748; Potkin SG, et al. Clin Psychopharmacoi. 2005;25(4):301-310; vieta E, et al. J Psychopharmacoi. 2010;24(4):547-558 |
| Adjunctive Therapy Trials | |
| Asenapine | Calabrese JR, et al. Asenapine as adjunctive treatment for bipolar mania: a placebo-controlled 12-week study and 40-week extension [poster). Presented at: European Psychiatric Association; February 27-March 2, 2010; Munich, Germany |
| Aripiprazole | Vieta E. et al. Am J Psychiatry. 2008;165(10):1316-1325 |
| Olanzapine | Tohen M, et al. Arch Gen Psychiatry. 2002;59(1):62-69; Houston JP, et al Clin Psychiatry. 2009;70(11):1540-1547 |
| Quetiapine | Sachs G, et al. Bipolar Disord. 2004;6(3):213-223; Yatham LN, et al. Int Clin psychopharmacoi. 2007;22(4):212-220 |
| Risperidone | Sachs GS, et al. Am J Psychiatry.2002:159(7): H46-1154;Yatham LN, et al. Br J Psychiatry. 2003;182:141-147 |
| Ziprasidone† | Weisler RH, et al. Ziprasidone in adjunctive treatment of acute bipolar mania: a randomized, placebo-controlled trial [poster]. Presented at: 16th congress of the European College of Neuropsychopharmacology; September 20-24, 2003; Prague, Czech Republic |
†All ziprasidone studies used the Mania Rating Scale.
‡Data are change from baseline ymrs at week 4 (Tohen et al. 2000 or week 6 (Tohen et al. 2002).
Results
Meta-analysis of Monotherapy Trials
Change In YMRS total score for asenapine monotherapy versus placebo is similar to that of other antipsychotics.
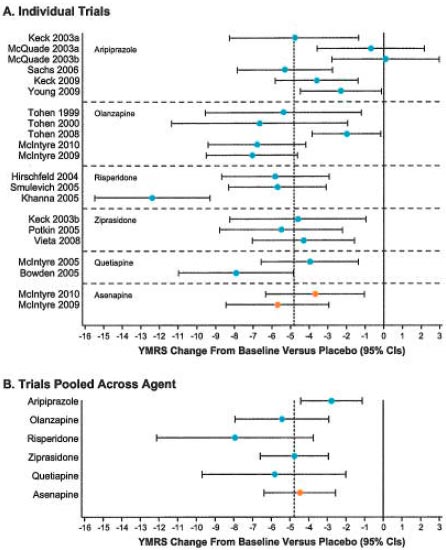
When combined, change from baseline ymrs total score at endpoint with asenapine exceeded that of placebo by 4.5 points (95% Cl, 2.5-6.4; P<0.0001).
Based on the Cochran Q statistic, the results across asenapine studies were homogenous (Q=0.7, df=1, P=0.41).
Change from baseline YMRS total score at endpoint among all pooled treatments exceeded that of placebo by 4.8 points (95% Cl, 3.7-6.0; p<0.0001); therefore, the asenapine treatment effect was comparable to that of the other antipsychotics.
There was considerable heterogeneity in treatment effect across studies (Q=69.5, df=19, P<0.001) owing to the results of 1 risperidone trial (Khanna et al. 2005) and 2 aripiprazole studies (McQuade 2003).
The potential source of heterogeneity due to a difference across compounds was discarded by an analysis that also included a factor for compound and studies nested within compounds (F(5,15)=1.58, p=0.23).
Additional post hoc meta-analyses reported no significant differences in mean YMRS change from baseline with asenapine monotherapy vs monotherapy with aripiprazole (1.9 [95% Cl, -0.9 to 4.7]), ziprasidone (-0.1 [95% Cl, -3.0 to 2.8]), risperidone (-3.3 [95% Cl, -8.3 to 1.7]), quetiapine (-1.1 [95% Cl, -4.5 to 2.2]), and olanzapine (-0.8 [95% Cl, -4.2 to 2.7]).
Meta-analysis of Adjunctive Therapy Trials
Change in YMRS total score for adjunctive asenapine versus placebo is similar to that of adjunctive therapy with other antipsychotics.
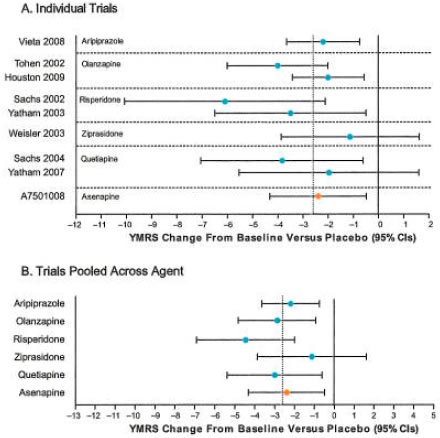
Change from baseline YMRS total score at endpoint with asenapine as an adjunct to lithium or valproate exceeded that of placebo by 2.4 points (95% Cl, 0.5-4.3; P=0.0257).
The overall efficacy of all pooled active agents exceeded that of placebo by 2.6 points (95% Cl, 1.9-3.3, P<0.0001), and the asenapine treatment effect was comparable to that of other antipsychotics.
The results across adjunctive therapy trials were homogeneous (Q=8.0, df=8, P=0.43).
Conclusions
The relative efficacy of asenapine vs placebo, as monotherapy or adjunctive therapy to lithium or valproate, is similar to that of other antipsychotics.
It should also be noted that some of the olanzapine studies were of longer duration (ie, 4 or 6 weeks), which may lead to their effect size being overestimated.
These meta-analyses have confirmed the statistically significant superior efficacy of asenapine vs placebo, as monotherapy or adjunctive therapy to lithium or valproate, for acute bipolar mania.
REFERENCES
1. Yildiz A, et al. Neuropsychopharmacol. 2011 ;36(2):375-89.
2. Scherk H, et al. Arch Gen Psychiatry. 2007;64(4):442-455.
3. Saphris® (asenapine sublingual tablets). Full Prescribing information, Schering Corporation, a subsidiary of Merck & Co., Inc, Whitehouse Station, NJ, 2010.
4. European Medicines Agency, Sycrest asenapine.
5. Mcintyre RS, et al. Bipolar Disord. 2009;11(7):673-686
6. Mcintyre RS, et al. J Affect Disord. 2010;122(1-2):27-38.
7. Calabrese JR, et al. Asenapine as adjunctive treatment for bipolar mania: a placebo-controlled 12-week study and 40-week extension. Presented at: European Psychiatric Association; February 27-March 2, 2010; Munich, Germany.
8. Perlis RH, et al. J Clin Psychiatry. 2006;67(4):509-516.
9. Dersimonian R and Laird N. Control Clin Trials. 1986;7(3):177-188.
10. van Houwelingen HC, et al. Stat Med. 2002;21(4):589-624.



